
Written By: Jeffrey Atlas, Health Content Writer
Medically Reviewed By: Dr. Gopal Grandhige, MD, FACS, Board-Certified Surgeon
Last Reviewed: May 30, 2026
If you’re dealing with acid reflux from chemo, the fastest relief usually comes from three things stacked together. Eat smaller meals sitting upright, sleep with your head elevated six to eight inches, and ask your oncology team whether your specific chemo drug interacts with antacids before you take anything. That last point is the one most patients miss, and it can cut your cancer medication’s effectiveness in half.
Roughly one in three to one in two people on chemotherapy develop reflux symptoms during treatment. That’s not a small side effect. It’s a wrecker. It steals sleep, kills appetite, and makes the nausea worse than it already is.
Here’s what we’ve seen at Tampa Bay Reflux Institute. Patients come in months after finishing chemo still battling daily heartburn, still on a PPI, and nobody has checked whether the reflux is from lingering tissue damage, a hiatal hernia that flared up, or something structural that no pill will fix. The fix isn’t always a stronger drug. Sometimes it’s an honest look at the anatomy.
What is acid reflux from chemo?
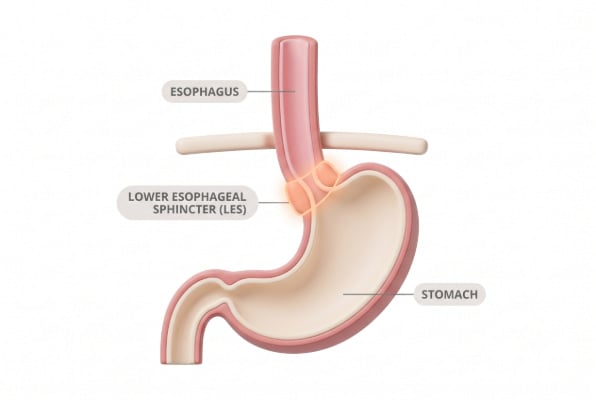
Acid reflux from chemo happens when chemotherapy drugs damage the rapidly dividing cells lining your esophagus, stomach, and the lower esophageal sphincter (LES), the muscle that’s supposed to keep stomach acid from rising. Once that muscle weakens or the lining gets inflamed, acid backs up into the esophagus, causing burning, regurgitation, coughing, and trouble swallowing. The condition can persist long after treatment ends.
That’s the citation-ready definition. Hold onto it because the rest of this piece breaks down what to do about it.
Why does chemotherapy trigger heartburn?
Chemo works by attacking fast-replicating cells. Cancer cells qualify. So do the cells lining your digestive tract, your hair follicles, and your bone marrow. The drugs can’t tell the difference.
When the esophagus gets hit, the tissue inflames. Doctors call this esophagitis. The inflammation can pull the LES out of position or weaken its grip. Stomach acid then leaks upward and burns the already-damaged tissue, which makes the inflammation worse. It’s a loop.
Some chemo drugs are worse for this than others. Cisplatin, doxorubicin, and methotrexate are notorious. Targeted therapies like erlotinib and dasatinib add another problem we’ll get to in the medications section.
Radiation to the chest or upper abdomen stacks on top of chemo and makes everything worse. If you’re getting both, expect reflux. Plan for it.
Who’s at higher risk?
You don’t need a long checklist to figure this out. If any of these describe you before chemo started, your reflux risk during treatment goes up:
- Overweight or carrying weight around the midsection
- Smoker or recent quitter
- Already had occasional heartburn before treatment
- Hiatal hernia (even a small one)
- Taking NSAIDs, corticosteroids, or certain antibiotics
- H. pylori infection in your history
- Pregnant (yes, some patients are)
The single biggest factor most people underestimate is a pre-existing hiatal hernia. Plenty of folks have a small one and don’t know it. Chemo nausea and vomiting can stretch and worsen that hernia, and suddenly the reflux gets dramatic. If you’ve had any history of regurgitation before treatment, mention it. A simple imaging study before chemo starts can flag this.

What foods help acid reflux from chemo?
Skip the giant “good foods/bad foods” chart and focus on what actually moves the needle. Johns Hopkins Medicine and other major centers agree on the basics, and the research backs them up.
Foods that tend to calm things down:
- Oatmeal and brown rice (high fiber, absorbs acid)
- Bananas, melons, apples, pears (low acid)
- Leafy greens, broccoli, green beans, zucchini
- Sweet potatoes, carrots
- Lean protein: skinless chicken, turkey, white fish, tofu
- Ginger (anti-inflammatory, settles the stomach)
- Plain water and chamomile tea
Foods that almost always make it worse:
- Coffee and caffeinated tea
- Chocolate
- Citrus fruits and juices (orange, grapefruit, lemon)
- Tomatoes and tomato sauce
- Onions, garlic, hot peppers
- Fried and fatty foods
- Carbonated drinks
- Peppermint
- Alcohol in any form
A note on ginger. It’s anti-inflammatory and helps most people, but roughly 5% of reflux patients find it makes things worse. If you try ginger tea and feel more burn, drop it. Listen to your own body over any list.
The one piece of advice that helps more than any specific food choice: eat five or six small meals instead of three big ones. A full stomach pushes acid up. A small one doesn’t.

How should I change my eating habits during chemo?
Five practical shifts that work better than any specific diet:
- Eat sitting upright. Reclining puts your stomach above your LES, which is backwards.
- Stop eating three hours before bed. Two hours minimum, three is better.
- Sleep on a wedge pillow or with the head of your bed raised six to eight inches. Stacking regular pillows doesn’t work because it bends you at the waist.
- Drink water with meals to dilute acid and help swallowing.
- Wear loose clothing. Anything that squeezes your waist pushes acid up.
That third one matters more than people realize. Sleeping flat is when most reflux damage happens, because gravity stops protecting you. A patient I worked with last year had been fighting nighttime reflux for six months on maximum-dose PPIs before anyone told her to elevate her bed. Two weeks later, she was sleeping through the night.
What medications work for chemo-related reflux?
Three classes of medication treat reflux, and they don’t all mix well with chemotherapy. This is where most articles glaze over the important part, so pay attention.
Antacids (Tums, Rolaids, Mylanta) neutralize acid that’s already in your stomach. They work fast, wear off fast, and are usually safe. Take them at least two hours apart from oral chemo drugs.
H2 blockers (Pepcid/famotidine, Tagamet/cimetidine) reduce acid production. They last longer than antacids. With oral chemo, separate the doses by at least 10 hours before and 2 hours after your cancer drug.
Proton pump inhibitors or PPIs (Nexium, Prilosec, Prevacid, Protonix) shut down acid production hard. They’re the strongest option and the one most patients end up on. They’re also the one with the biggest problem during chemo.
Here’s the contrarian take that needs to land. PPIs are massively overprescribed, and during chemo they can be dangerous. Some oral chemotherapy drugs, including dasatinib (Sprycel) and erlotinib, require stomach acid to absorb properly. Published research has shown that taking a PPI alongside these drugs can drop blood levels of the cancer medication by up to 50%. You’re treating a side effect by weakening the treatment.
If your oncologist hasn’t checked your specific drug list against your reflux meds, ask them to. Today.
About 40 to 55% of GERD patients on optimal PPI therapy still have symptoms. That’s not me cherry-picking, that’s the consensus number from gastroenterology research. So even when PPIs are safe to take, they don’t work for everyone.
Can chemo cause permanent acid reflux?
Yes, and this is the part nobody warns you about up front. The tissue damage from chemo usually heals, but the structural changes don’t always reverse. A weakened LES can stay weak. A hiatal hernia that flared up during treatment doesn’t shrink back down. Esophagitis can become a chronic problem.
This is why post-chemo reflux is its own conversation. If you’re three months past your last infusion and still on a daily PPI, something deeper is going on. That’s the point where a foregut specialist actually matters, not your primary care doctor and not your oncologist.

When should surgery enter the conversation?
Most articles bury this topic or write it off entirely. That’s a mistake. For the right patient, surgery is the closest thing to a permanent fix that exists.
Dr. Gopal Grandhige and the foregut surgeons at Tampa Bay Reflux Institute see this pattern constantly. Cancer survivor, finished treatment six to twelve months ago, still battling daily reflux, still on a PPI, often dealing with a hiatal hernia that needs repair anyway. The options at that point:
- Fundoplication wraps part of the stomach around the LES to reinforce it. Works for severe reflux and large hernias.
- LINX uses a small ring of magnetic beads to support the LES. Reversible. Good for moderate cases.
- TIF rebuilds the valve from inside the esophagus. No incisions. Recovery in days.
A 2025 five-year study on newer anti-reflux devices showed over 90% improvement in quality-of-life scores and only 2.1% of patients still needed PPIs at follow-up. Compare that to 40-55% who fail PPI therapy and stay on it forever anyway.
Not every chemo survivor needs surgery. But every chemo survivor with persistent reflux should at least get evaluated. Proper workup includes pH testing, manometry to check esophageal motility, and imaging for hiatal hernia. Without that workup, you’re guessing.
When should I call my doctor versus my GI specialist?
Call your oncologist immediately for: blood in vomit or stool, chest pain that feels different from heartburn, trouble breathing, severe pain swallowing, or any new symptom during active treatment.
Call a foregut specialist when: reflux persists more than three months after chemo ends, PPIs aren’t working, you’ve developed regurgitation or chronic cough, swallowing food feels harder than it should, or your GERD symptoms are interfering with sleep or eating.
The middle ground (mild heartburn, occasional regurgitation, manageable with diet) can usually go through your primary doctor. The line in the sand is whether reflux is controlling your life or you’re controlling it.
What about silent reflux after chemo?
Silent reflux, also called LPR (laryngopharyngeal reflux), is the version that doesn’t burn. Instead it gives you a chronic cough, a hoarse voice, the sensation of a lump in your throat, or postnasal drip that won’t quit. It’s frequently missed after chemo because everyone’s looking for classic heartburn.
If you finished treatment six months ago and your voice still sounds rough or you keep clearing your throat, this is probably what’s happening. LPR often involves non-acid reflux, which means PPIs may not help at all. Specific testing matters here, and it’s another reason a foregut workup makes sense.
The bottom line on chemo and reflux
Diet and lifestyle changes handle the majority of chemo-related heartburn. Medications fill in the rest, with the giant caveat that you must check interactions with your oncologist first. And if reflux outlasts your treatment, stop accepting “just take a PPI forever” as the answer. Get the workup. Find out if there’s a structural fix.
Tampa Bay Reflux Institute helps you eliminate reflux and GERD when standard treatment stops cutting it.
FAQs
Can chemotherapy cause permanent acid reflux?
Yes. Chemo can permanently weaken the lower esophageal sphincter and worsen pre-existing hiatal hernias, leading to chronic GERD even after treatment ends. About one in three to one in two chemo patients develop reflux during treatment, and a significant portion still have symptoms a year later. Persistent post-chemo reflux usually means there’s a structural issue worth investigating.
What’s the best position to sleep in with chemo reflux?
Sleep on your left side with the head of your bed raised six to eight inches. Wedge pillows work, but stacking regular pillows doesn’t because it folds your body at the waist instead of elevating your torso. Left-side sleeping keeps the stomach below the esophagus and reduces nighttime reflux significantly.
Can I take Tums during chemotherapy?
Usually yes, but timing matters. Antacids like Tums neutralize stomach acid and can reduce absorption of certain oral chemo drugs by up to 50%. Take antacids at least two hours apart from your cancer medications, and confirm the specific timing with your oncologist or pharmacist.
Is acid reflux from chemo different from regular GERD?
The mechanism is similar but the causes differ. Regular GERD usually comes from a weakened LES or hiatal hernia developing slowly over years. Chemo reflux comes from direct tissue damage to the digestive tract lining and can develop within days of starting treatment. The treatments overlap, but chemo patients have extra considerations around drug interactions.
How long does chemo-induced acid reflux last?
Most patients see improvement within four to eight weeks after their final chemo session as the digestive tissue heals. But roughly 30% of patients have lingering reflux symptoms six months out, often because of structural changes that don’t reverse on their own. If you’re still battling daily heartburn three months post-treatment, get evaluated.
Do I need surgery for acid reflux after chemo?
Most patients don’t, but some absolutely should consider it. Candidates include anyone with a confirmed hiatal hernia, patients who fail PPI therapy, those dealing with regurgitation rather than just burning, and cancer survivors who can’t safely stay on long-term acid-suppressing drugs. A proper workup with pH testing and manometry sorts out who benefits.
What foods should I avoid with acid reflux from chemo?
Skip coffee, chocolate, citrus, tomatoes, fried foods, alcohol, carbonated drinks, peppermint, raw onions, garlic, and hot peppers. These either relax the LES or directly irritate inflamed esophageal tissue. Focus instead on oatmeal, bananas, melons, lean proteins, leafy greens, and ginger.

{kind=link}
{kind=link}

An endoscopy cannot tell you if you have reflux. It can only tell you if you have complications of GERD.
If you are unhappy with your reflux symptoms, come in and we can discuss testing and treatments that can accurately diagnose your problem.
#reflux #gerd #hiatalhernia #gastroparesis #linx
{kind=link}

CALL US AT 813-922-2920
www.tampareflux.com
If you have a hiatal hernia and fit one of these categories, you should know your options.
Dr. Grandhige is an expert in his field and performs 200 of these surgeries a year. He is the only surgeon in the Tampa Bay Area who offers all surgical options - LINX, Fundoplications, TIF and will be one of 20 surgeons in America introducing the latest procedure RefluxStop in 2026.
We accept most insurances but will verify yours before you come in. These procedures are considered medically necessary and covered by your insurance. You can expect to pay your in-network deductibles and nothing else.
#hiatalhernia #reflux #GERD #LINX #refluxstop
{kind=link}
What causes reflux ?
1. Weak lower esophageal sphincter
2. Hiatal hernia
3. Flattening of the Angle of His
4. Poor esophageal motility
5. Gastroparesis (slow stomach)
NOT increased acid production
{kind=link}
{kind=link}
Don’t let GERD get in the way of living your life. Request your appointment with us today on the link below.
.
.
.
.
https://tampareflux.com/contact-us/
{kind=link}
Anyone can be victim to GERD and though weight loss can help reduce GERD symptoms. Many athletes with high impact workouts may continue to have these symptoms. This may be a symptom of a hiatal hernia or other issue. We are more then happy to assist you in finding your solution, just click the link below.
.
.
.
https://tampareflux.com/contact-us/
##healthylifestyle #workout #athletereflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
Heartburn may seem like an annoyance. But if you find yourself having symptoms on a daily basis, it may be time to to talk to Dr. Grandhige as it could be a symptom of something worse.
.
.
.
#chronicheartburn #gerdsymptoms #heartburnrelief #reflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
If you are tired of avoiding your favorite foods or taking daily medications, we can help.
We are the Tampa experts in reflux ! With years of experience and thousands of patients treated successfully, we offer all FDA approved anti-reflux procedures.
Call 813-922-2920 to schedule your appointment
All major insurances accepted.
{kind=link}
Not all patients need surgical intervention. Many patients are living a heartburn free life with their PPIs. However 40% of patients taking PPIs are not getting the relief they need. If you are one of those, you have options! Come in and find out more.
.
.
.
.
#letushelpyou #medsnotworking #reflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
#heartburn #stopreflux #hiatalherniarepair #severeheartburn #reflux #tampabayreflux #acidrefluxsurgery #tampaheartburn #GERD #PPIs #achalasia #LINX #TIF #tampareflux #fundoplication #stomach #digestivehealth #ESG #obesity #overweight #weightlossjourney #gastricballoon
{kind=link}