
Written By: Dr. Ahmad Saad, Health Content Writer
Medically Reviewed By: Dr. Gopal Grandhige, MD, FACS, Board-Certified Surgeon
Last Reviewed: January 25, 2026
Gastroparesis is a chronic stomach disorder where the stomach empties food too slowly into the small intestine without any physical blockage present. Affecting approximately 25 per 100,000 people, with actual numbers likely much higher due to underdiagnosis, this condition causes debilitating symptoms including persistent nausea, vomiting, early fullness after eating, and upper abdominal pain.
Women are four times more likely to develop gastroparesis than men, and the condition stems primarily from three causes: diabetes (25% of cases), unknown origins (idiopathic), and post-surgical complications. The gold standard for diagnosis is gastric-emptying scintigraphy (GES), a specialized imaging test that tracks how long food remains in the stomach.
Understanding gastroparesis is crucial because early recognition and proper management, ranging from dietary modifications to FDA-approved medications and advanced interventions, can significantly improve quality of life. This comprehensive guide covers the 10 essential facts every patient and caregiver needs to know about gastroparesis symptoms, causes, diagnosis methods, treatment options, and when to seek emergency care.
1. The Tell-Tale Symptoms You Shouldn’t Ignore
This condition triggers various gastrointestinal manifestations. Those affected by gastroparesis typically experience nausea, vomiting, early feelings of fullness, post-meal discomfort, bloating, and pain in the upper abdomen.3 Recognizing these symptoms early can help you seek appropriate medical attention and begin treatment sooner. Many of these digestive symptoms overlap with other conditions like GERD and silent reflux, making accurate diagnosis essential. According to the Mayo Clinic, persistent symptoms warrant immediate medical evaluation to prevent complications.
2. The Three Main Causes of Gastroparesis
Three primary factors contribute to the development of gastroparesis. Diabetes, post-operative complications, and idiopathic origins stand as the leading causes of this condition. Between them, diabetes and idiopathic cases represent over 60 percent of documented instances, with diabetes mellitus specifically responsible for roughly 25 percent of cases. Additional gastroparesis triggers encompass connective tissue disorders, autoimmune conditions, ischemia, and certain medications that decelerate gastric emptying. Such medications include opioid pain relievers, contemporary diabetic drugs, antidepressants, anticholinergic agents, and blood pressure medications. In pediatric populations, gastroparesis diagnosis frequently goes unrecognized, though most childhood cases stem from viral infections or surgical procedures.1,4–7 The National Institute of Diabetes and Digestive and Kidney Diseases provides comprehensive information about how diabetes affects gastric motility.

3. How Doctors Diagnose Gastroparesis
Gastric-emptying scintigraphy (GES) serves as the primary diagnostic method for gastroparesis. This procedure requires patients to consume a radiolabeled meal, typically containing eggs, followed by imaging at various intervals to assess gastric retention levels. Upper endoscopy is additionally conducted during the diagnostic workup to rule out mechanical (obstructive) factors. Alternative diagnostic approaches include breath testing, wireless capsule motility assessment, and antro-duodenal motility studies, though these are less frequently employed. Breath testing offers a non-invasive option suitable for outpatient settings, involving the combination of a 13C isotope attached to octanoic acid (a digestible compound) with a solid meal. Following consumption, 13C-CO2 metabolism can be tracked through exhaled breath from the lungs. While this method benefits from avoiding ionizing radiation exposure, it cannot be used for patients with celiac disease or lactose intolerance.8,9 Cleveland Clinic experts emphasize the importance of comprehensive testing to distinguish gastroparesis from other digestive disorders.
4. Women Are Four Times More Likely to Be Affected
Women experience gastroparesis at higher rates than men, and while uncommon, the condition can emerge during childhood. A comprehensive population-based study examining gastroparesis revealed age-adjusted incidence rates for definite gastroparesis of 2.4 per 100,000 person-years among men compared to 9.8 per 100,000 person-years among women. Furthermore, definitive gastroparesis prevalence reached 9.6 per 100,000 person-years in men and 38 per 100,000 person-years in women. Among children, gastroparesis cases show more balanced gender distribution, with slightly higher occurrences in male children and female adolescents. Pediatric and adolescent patients less frequently report abdominal pain, nausea, and bloating, while early fullness and weight loss are more commonly observed. Premature infants frequently demonstrate delayed gastric emptying, which typically resolves with maturation (generally by 32 weeks gestation).7,10,11 Johns Hopkins Medicine researchers continue to study why women are disproportionately affected by this condition.
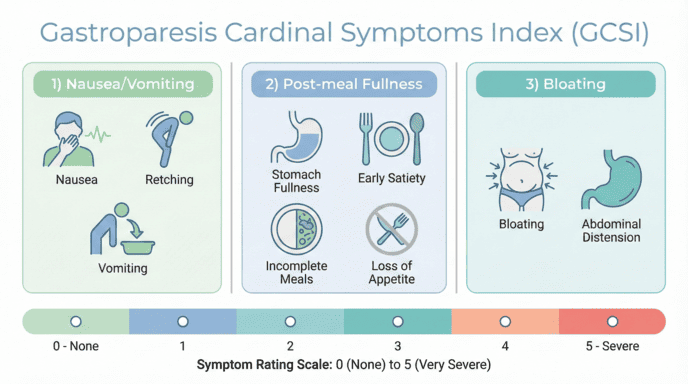
5. The GCSI: Measuring Your Symptom Severity
The Gastroparesis Cardinal Symptoms Index (GCSI) was created to measure symptom severity in affected patients. This index divides into three sections: nausea/vomiting, post-meal fullness/early satiety, and bloating.12 Patients rate each criterion from 0 to 5, where 0 indicates symptom absence and 5 denotes very severe manifestations. The nausea/vomiting section encompasses three criteria: nausea, retching, and vomiting. The post-meal fullness/early satiety section contains four criteria: stomach fullness, inability to complete meals, fullness following eating, and appetite loss. The bloating section includes two criteria: bloating and visible abdominal enlargement. Tracking patients’ GCSI scores enables clinicians to assess whether symptoms are improving or deteriorating over time. Harvard Health recommends keeping a symptom diary to help healthcare providers monitor disease progression.
6. Not Everything That Looks Like Gastroparesis Actually Is
Several important differential diagnoses that produce chronic nausea and vomiting must be excluded when diagnosing gastroparesis. Various psychiatric conditions including depression and eating disorders can present with clinical manifestations resembling gastroparesis. Rumination syndrome involves daily regurgitation of undigested food shortly after consumption, yet these individuals maintain normal gastric emptying function. Functional dyspepsia shares overlapping symptoms like early fullness sensations and bloating, though dyspepsia patients typically demonstrate normal emptying, with only one-third showing delayed emptying.13 Conditions like achalasia and hiatal hernias may also present with similar symptoms, requiring careful evaluation by specialized reflux doctors. Learn more about our approach to diagnosing complex digestive conditions.
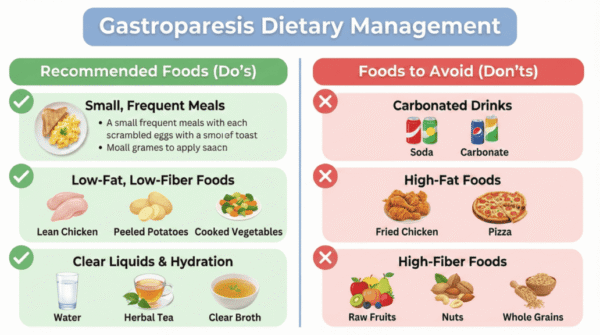
7. Dietary Changes Are the First Line of Treatment
Given the potential adverse effects of medications, dietary modifications are typically the first-line approach for both children and adults. Consuming frequent, smaller meals that minimize fat and fiber content is advised, as these components contribute to delayed gastric emptying. Patients should also eliminate carbonated beverages and maintain adequate hydration. Liquid diets are often better tolerated since gastroparesis typically impacts solid food emptying more than liquids. When liquids prove intolerable, enteral nutrition may become necessary to prevent caloric deficiency. For patients experiencing significant weight loss, incisionless weight loss procedures may be considered as part of comprehensive digestive health management. Metoclopramide currently stands as the sole FDA-approved medication for gastroparesis treatment. This drug functions as a dopamine D2-receptor antagonist. Since dopamine produces a relaxing effect on the gastrointestinal tract, blocking it promotes motility. Anti-emetic medications address nausea and vomiting symptoms (ondansetron, promethazine, scopolamine). Elevated blood sugar can worsen gastric emptying delays, making glycemic control beneficial for symptom management.3,7,14 WebMD offers practical dietary guidelines for managing gastroparesis symptoms effectively.
8. Understanding Medication Options and Side Effects
Metoclopramide’s typical side effects may include altered taste perception, headaches, and fatigue. Prolonged metoclopramide use carries increased risk for developing tardive dyskinesia and Parkinson-like syndrome. While not FDA-approved for pediatric use, metoclopramide remains commonly prescribed in pediatric management. Numerous ongoing trials are investigating the risks and benefits of metoclopramide in children. The FDA has approved promethazine only for children over age 2. The agency advises cautious use at minimal doses due to documented cases of respiratory depression and fatalities. Additional gastroparesis drugs remain in clinical trial phases, with none yet demonstrating sufficient efficacy for FDA approval. The American College of Gastroenterology provides updated guidelines on medication management for gastroparesis patients. Patients with coexisting conditions may benefit from treatments addressing abdominal hernia and heartburn symptoms.
9. Advanced Options When Standard Treatments Fail
Endoscopic and surgical interventions exist for gastroparesis treatment. Roughly 30 percent of gastroparesis patients fail to achieve symptom relief through less invasive approaches like dietary changes and medications. For this patient population, endoscopic and surgical alternatives warrant discussion. Endoscopic procedures include botulinum toxin (Botox) injection into the pylorus and G-POEM (endoscopic pyloroplasty). Surgical interventions encompass gastric stimulator implantation, surgical pyloroplasty, and subtotal gastrectomy. Enterra Therapy utilizing an electric gastric stimulator represents an approved treatment for mechanical stomach stimulation. This device can be implanted through open surgery or laparoscopic technique. During the procedure, two electrodes attach to the stomach’s greater curvature approximately 10 cm from the pylorus, with the opposite ends connecting to the neurostimulator. The stimulator is surgically secured beneath the skin in the abdominal wall, and initial device parameters are established.15 Periodic reprogramming of the device occurs in clinical settings based on individual patient requirements. Tampa Reflux Center offers advanced surgical treatments including fundoplication surgery, LINX procedure, and transoral incisionless fundoplication for complex digestive disorders.
10. Emergency Care and Home Support Can Make a Difference
Certain adjunctive therapies merit consideration for patients experiencing poor outcomes and substantial weight loss. Gastroparesis patients demonstrate positive responses to single-dose haloperidol administration in emergency settings. Single haloperidol doses have been shown to significantly decrease hospital admission rates and opiate requirements within emergency departments. Patients experiencing considerable gastrointestinal losses should be evaluated for home intravenous fluids/total parenteral nutrition or enteral feeding via tube. Access to supplemental fluids or nutrition at home can reduce hospitalization frequency. MedlinePlus offers resources for patients seeking emergency care guidelines and home management strategies.
Conclusion
Gastroparesis is a complex digestive disorder that affects thousands of individuals, with many cases remaining undiagnosed due to lack of awareness about its symptoms. Understanding the characteristic signs such as nausea, vomiting, early fullness, and upper abdominal pain is crucial for seeking timely medical intervention. While the condition disproportionately affects women and commonly stems from diabetes or remains idiopathic in origin, proper diagnosis through gastric-emptying scintigraphy and comprehensive evaluation can lead to effective management strategies.
Treatment approaches range from dietary modifications as the first line of defense to FDA-approved medications like metoclopramide, and in more severe cases, advanced interventions including endoscopic procedures or surgical options. The key to successful gastroparesis management lies in early recognition, accurate diagnosis, individualized treatment plans, and ongoing monitoring of symptom severity. With appropriate medical care, lifestyle adjustments, and when necessary, advanced therapeutic interventions, patients with gastroparesis can achieve better symptom control and improved quality of life. For more information about comprehensive gastroparesis care or to explore related digestive health topics, visit our medical blog or schedule a consultation with our specialists. Additional evidence-based resources are available through Healthline and the National Center for Biotechnology Information.
FAQs
What is gastroparesis and what causes it?
Gastroparesis is a stomach disorder characterized by delayed gastric emptying without mechanical blockage. The three main causes are diabetes, post-surgical complications, and idiopathic origins, with diabetes and idiopathic cases accounting for over 60% of all instances.
How is gastroparesis diagnosed?
Gastric-emptying scintigraphy (GES) is the primary diagnostic method, where patients consume a radiolabeled meal and undergo imaging to assess gastric retention. Upper endoscopy is also performed to rule out any mechanical obstructions in the digestive tract.
What are the main symptoms of gastroparesis?
Common symptoms include nausea, vomiting, early feelings of fullness after eating, post-meal discomfort, bloating, and upper abdominal pain. These symptoms occur because the stomach takes too long to empty its contents into the small intestine.
What dietary changes help manage gastroparesis?
Patients should eat frequent, smaller meals that are low in fat and fiber, as these slow gastric emptying. Liquid diets are often better tolerated than solid foods, and staying well-hydrated while avoiding carbonated beverages is recommended.
Is metoclopramide safe for long-term use?
Metoclopramide is the only FDA-approved medication for gastroparesis but carries risks with prolonged use, including tardive dyskinesia and Parkinson-like syndrome. Patients should discuss the benefits and risks with their healthcare provider and use it at the lowest effective dose.

{kind=link}
{kind=link}

An endoscopy cannot tell you if you have reflux. It can only tell you if you have complications of GERD.
If you are unhappy with your reflux symptoms, come in and we can discuss testing and treatments that can accurately diagnose your problem.
#reflux #gerd #hiatalhernia #gastroparesis #linx
{kind=link}

CALL US AT 813-922-2920
www.tampareflux.com
If you have a hiatal hernia and fit one of these categories, you should know your options.
Dr. Grandhige is an expert in his field and performs 200 of these surgeries a year. He is the only surgeon in the Tampa Bay Area who offers all surgical options - LINX, Fundoplications, TIF and will be one of 20 surgeons in America introducing the latest procedure RefluxStop in 2026.
We accept most insurances but will verify yours before you come in. These procedures are considered medically necessary and covered by your insurance. You can expect to pay your in-network deductibles and nothing else.
#hiatalhernia #reflux #GERD #LINX #refluxstop
{kind=link}
What causes reflux ?
1. Weak lower esophageal sphincter
2. Hiatal hernia
3. Flattening of the Angle of His
4. Poor esophageal motility
5. Gastroparesis (slow stomach)
NOT increased acid production
{kind=link}
{kind=link}
Don’t let GERD get in the way of living your life. Request your appointment with us today on the link below.
.
.
.
.
https://tampareflux.com/contact-us/
{kind=link}
Anyone can be victim to GERD and though weight loss can help reduce GERD symptoms. Many athletes with high impact workouts may continue to have these symptoms. This may be a symptom of a hiatal hernia or other issue. We are more then happy to assist you in finding your solution, just click the link below.
.
.
.
https://tampareflux.com/contact-us/
##healthylifestyle #workout #athletereflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
Heartburn may seem like an annoyance. But if you find yourself having symptoms on a daily basis, it may be time to to talk to Dr. Grandhige as it could be a symptom of something worse.
.
.
.
#chronicheartburn #gerdsymptoms #heartburnrelief #reflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
If you are tired of avoiding your favorite foods or taking daily medications, we can help.
We are the Tampa experts in reflux ! With years of experience and thousands of patients treated successfully, we offer all FDA approved anti-reflux procedures.
Call 813-922-2920 to schedule your appointment
All major insurances accepted.
{kind=link}
Not all patients need surgical intervention. Many patients are living a heartburn free life with their PPIs. However 40% of patients taking PPIs are not getting the relief they need. If you are one of those, you have options! Come in and find out more.
.
.
.
.
#letushelpyou #medsnotworking #reflux #PPIs #heartburn #LINX #fundoplication #TIF #GERD#tampaheartburn #linx #TIF #fundoplication #tampabayreflux #GERD #acidreflux #acidrefluxsurgery #stopreflux
#nonsurgicalweightloss #ESG #gastricballoon #weightlossjourney #vsg #vsgjourney #spatz3 #orbera #orberaballoon #grandhige #DrG
#tampabayrefluxinstitute #guthealth #roboticsurgery
{kind=link}
#heartburn #stopreflux #hiatalherniarepair #severeheartburn #reflux #tampabayreflux #acidrefluxsurgery #tampaheartburn #GERD #PPIs #achalasia #LINX #TIF #tampareflux #fundoplication #stomach #digestivehealth #ESG #obesity #overweight #weightlossjourney #gastricballoon
{kind=link}